Posted verbatim in all its glory. This is great news.
98th National Convention of the AMERICAN LEGION held in Cincinnati, Ohio on August 30, 31, September 1, 2016
Resolution No. 11: Medical Marijuana Research Origin: Louisiana Submitted by:
Convention Committee on Veterans Affairs & Rehabilitation
WHEREAS, Over the past several years, post-traumatic stress disorder (PTSD) and traumatic brain injury (TBI) have been thrust into the forefront of the consciousness of the medical community and the general public in large part due to recent combat operations and subsequent recognition of these potentially ‘silent injuries”; and
WHEREAS, Our foundation of knowledge guiding current diagnostics and interventions of PTSD and TBI has gained through decades of study in the academic medical world; and
WHEREAS, PTSD and TBI produce a complex constellation of medical consequences including physical, emotional, behavioral, and cognitive deficits; and
WHEREAS, The impact is heterogeneous given the varied types of injury (closed, penetrating, blast), severity, comorbid conditions, and premorbid characteristics; and
WHEREAS, The Department of Defense (DoD) and the Department of Veteran Affairs (VA) (May 2007), by consensus, have defined traumatic brain injury as any traumatically induced structural injury and/or physiological disruption of brain function as a result of an external force that is indicated by new onset or worsening of at least one of the following clinical signs, immediately following the event:
1. Any period of loss of or a decreased level of consciousness;
2. Any loss of memory for events immediately before or after the injury;
3. Any alteration in mental state at the time of the injury (e.g., confusion, disorientation, slowed thinking);
4. Neurological deficits (e.g., weakness, balance disturbance, praxis, paresis/plegia, change in vision, other sensory alterations, aphasia) that may or may not be transient;
5. Intracranial lesions; and
WHEREAS, TBI is a leading cause of death and disability in the United States where one and a half million Americans incur a traumatic brain injury (TBI) each year 9CDC, 2007); and
WHEREAS, These figures likely underestimate the true incidence of military injuries and those with mid injuries may not seek health care; and
WHEREAS, Direct costs for hospital care, extended care, and other medical care and services, coupled with indirect costs such as lost productivity were estimated at $60 billion annually in 2000 (CDC 2007; Finkelstein et al., 2006); and
WHEREAS, These figures do not include the physical, emotional, and social costs to the injured persons and their family from TBI-related disability; and
WHEREAS, For fiscal year 2009, there were 1, 313 veterans who received VA inpatient hospital care for TBI; and
WHEREAS, The Department of Veteran Affairs defines PTSD as a psychiatric disorder that can occur following the experience or witnessing of life-threatening events such as military combat, natural disasters, terrorist incidents, serious accidents, or violent personal assaults like rape; and
WHEREAS, From April 2007 through fiscal year 2009, thousands of veterans were identified as possibly having PTSD or a TBI through outpatient screening of individuals presenting to the VA for health care following deployment in Operation Enduring Freedom or Operation Iraqi Freedom; and
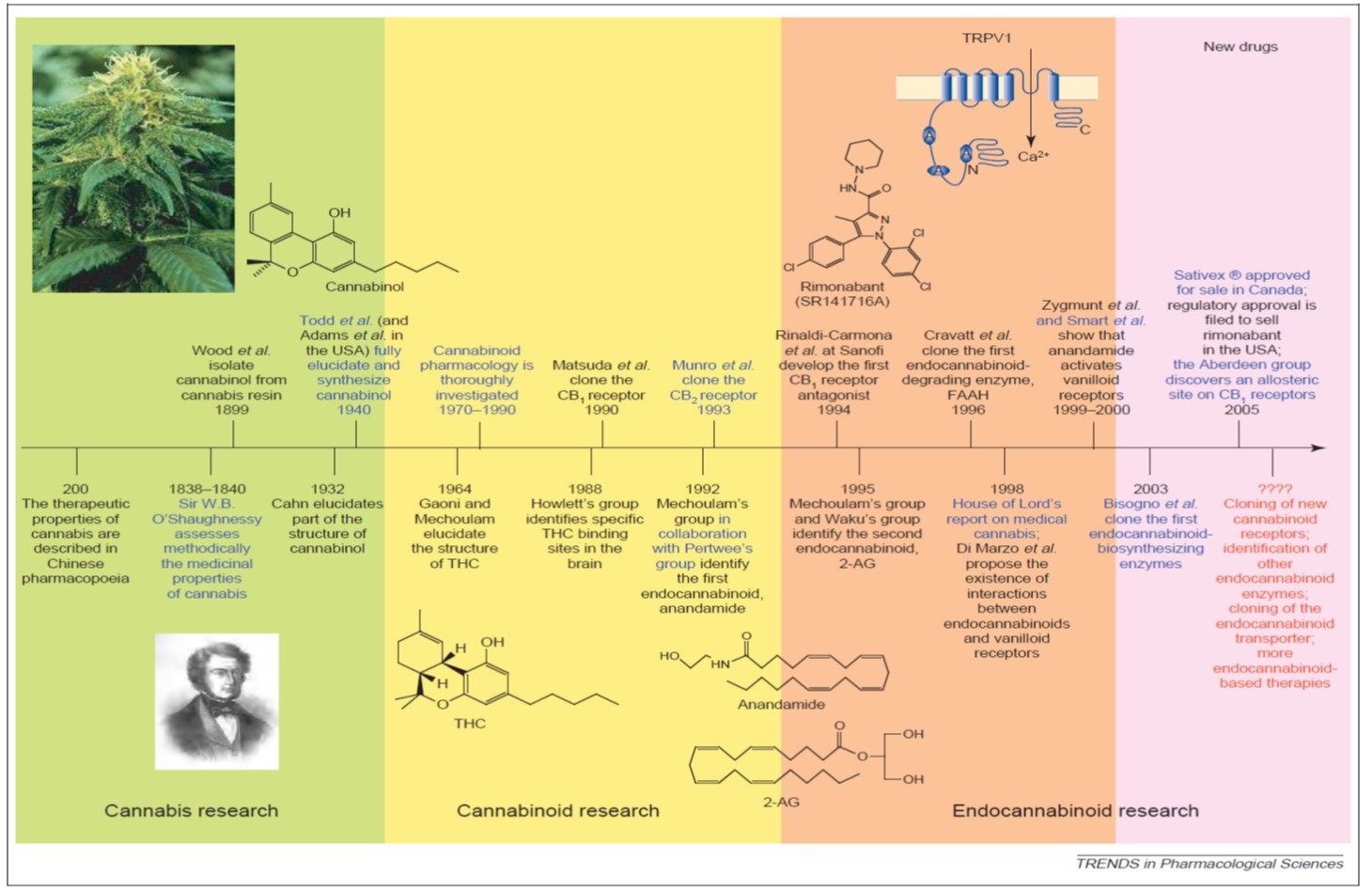
WHEREAS, About 20 years ago, scientist discovered a system in the brain called the endocannabinoid system that responds to 60 chemicals in marijuana, also known as cannabis; and
WHEREAS, This system plays a role in many of the body’s functions, such as in the heart, along with the digestive, endocrine, immune, nervous, and reproductive systems; and
WHEREAS, This discovery sparked interest in finding specific chemicals made from marijuana that could be targeted for specific conditions; and
WHEREAS, Marijuana is classified as schedule I drugs and drugs such as cocaine, methamphetamine, methadone, hydromorphone (Dilaudid), meperidine (Demerol), oxycodone (OxyContin), fentanyl, Dexedrine, Adderall, and Ritalin are classified as schedule II drugs; and
WHEREAS, In April 2016, the Drug Enforcement Agency gave its approval to a study on the effect of medical marijuana on post-traumatic stress disorder, the first randomized, controlled research in the U.S. for PTSD that will use the actual plant instead of oils or synthesized cannabis; now, therefore, be it
RESOLVED, By The American Legion in National Convention assembled in Cincinnati, Ohio, August 30, 31, September 1, 2016, that The American Legion urge the Drug Enforcement Agency to license privately-funded medical marijuana production operations in the United States to enable safe and efficient cannabis drug development research; and, be it finally,
RESOLVED, That The American Legion urge Congress to amend legislation to remove Marijuana from schedule I and reclassify it in a category that, at a minimum will recognize cannabis as a drug with potential medical value.





































{kind=link}